




La insuficiencia cardiaca (Killip>I) en pacientes con síndrome coronario agudo (SCA) es un reconocido factor de riesgo para mortalidad; sin embargo, su relación con la aparición de nuevos episodios isquémicos agudos no ha sido bien establecida.
ObjetivoEl objetivo del presente trabajo fue evaluar la asociación entre Killip>I al ingreso y la aparición de infarto agudo de miocardio (IAM) tras el alta hospitalaria por SCA.
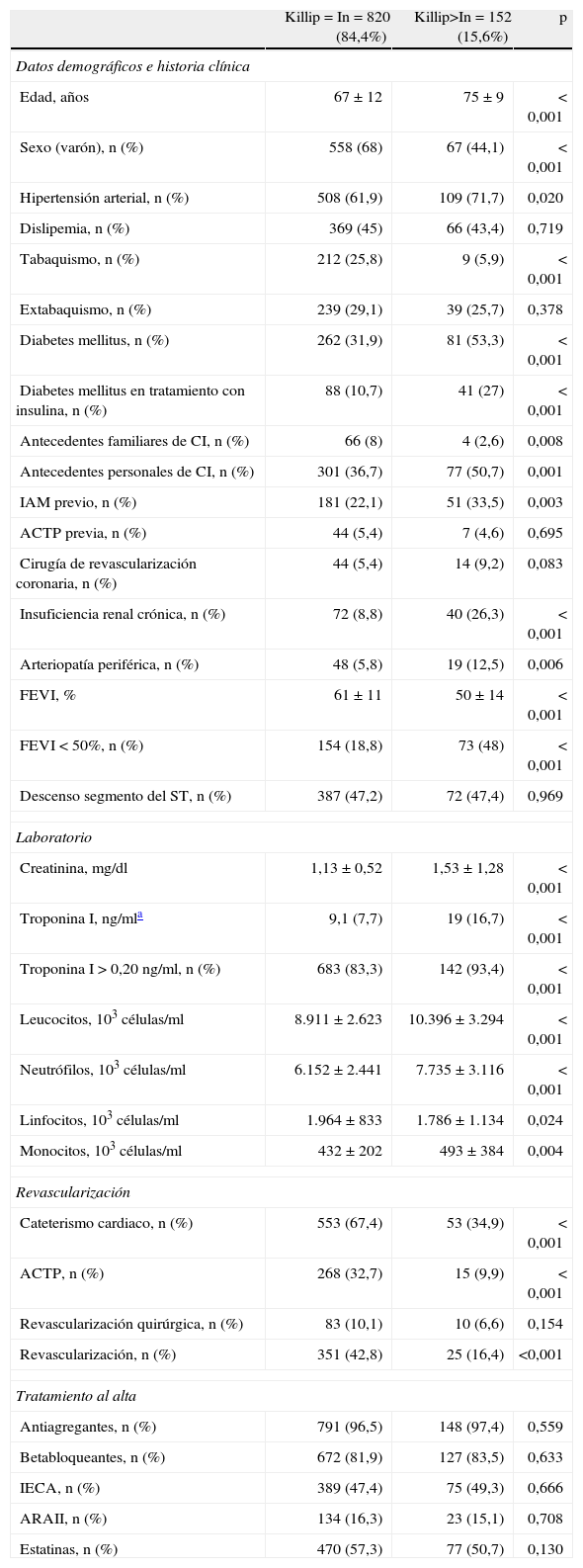
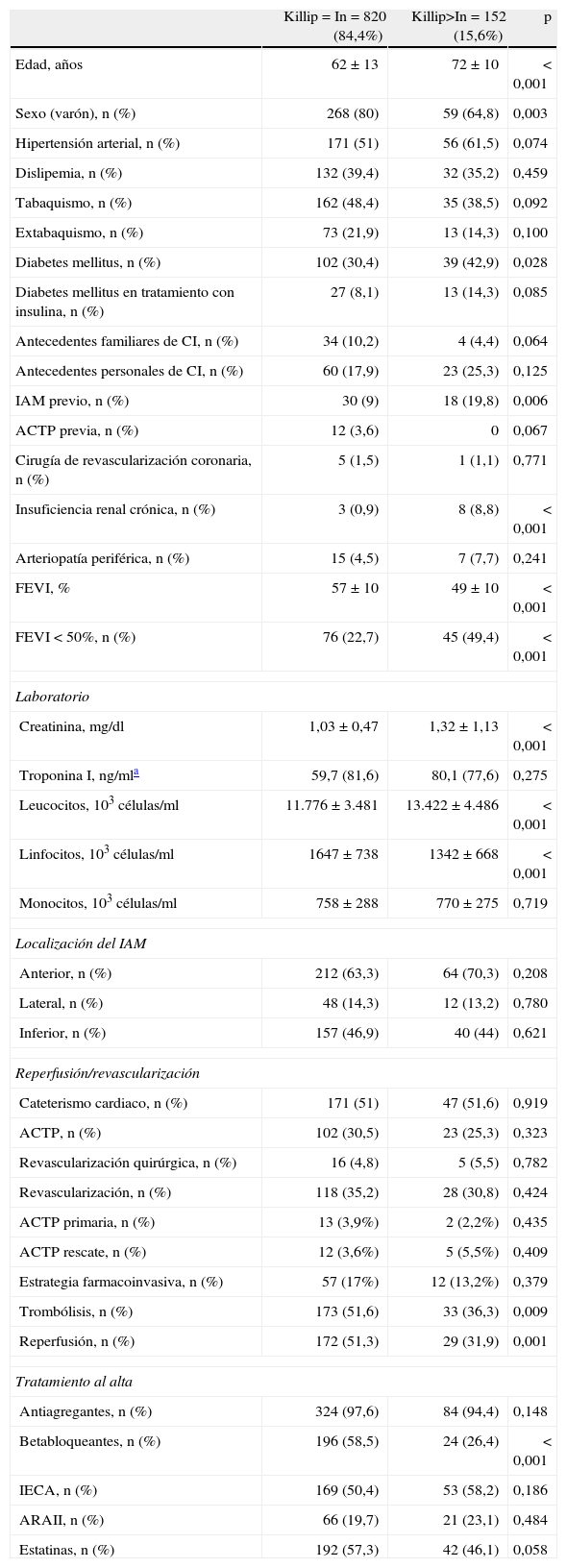
Pacientes y métodosSe estudió de forma prospectiva y consecutiva 972 y 426 supervivientes a un SCA sin elevación del segmento ST (SCASEST) e IAM con elevación del segmento ST (IAMCEST) respectivamente. Se determinó la presencia de Killip>I en el momento del ingreso junto con variables pronósticas clásicas. La asociación entre Killip>I e IAM se determinó mediante regresión de Cox adaptada para episodios competitivos.
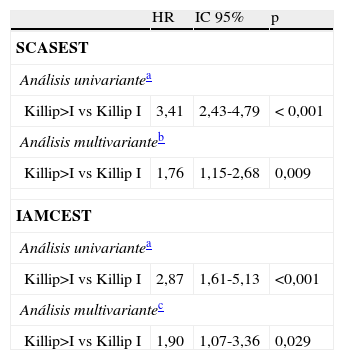
ResultadosDurante una mediana de seguimiento de 3 años, 135 (13,9%) y 53 (12,4%) pacientes con SCASEST y IAMCEST presentaron un IAM. Los pacientes con SCASEST y IAMCEST con Killip>I (15,6 y 21,3% respectivamente) presentaron más frecuentemente IAM (28,3 vs 6,3 y 10,6 vs 3,3 por 100 pacientes-año seguimiento, p<0,001 respectivamente). El análisis multivariante, ajustado por factores de riesgo y controlado por episodios competitivos (muerte y revascularización), confirmó que el SCASEST y IAMCEST Killip>I mostraron un incremento en el riesgo de IAM (HR=1,76; IC 95%: 1,15-2,68; p<0,009 y HR=1,90; IC 95%: 1,07-3,36; p=0,029 respectivamente).
ConclusionesEn pacientes con SCASEST y IAMCEST, la presencia de Killip>I al ingreso se asocia de manera independiente con mayor riego de IAM en el seguimiento.
Heart failure (Killip>I) in patients with acute coronary syndrome (ACS) is a recognized risk factor for death. However, its relationship with the risk of new acute ischemic events has not been well established.
ObjectiveThe aim of this study has been to evaluate the association between Killip>I on admission and the risk of a new acute myocardial infarction (AMI) during follow-up due to ACS.
Patients and methodsA total of 972 and 426 survivors of an ACS with non-ST segment evaluation (Non-STE-ACS) and AMI with ST segment elevation (STEMI) were studied prospectively and consecutively. The presence of Killip>I was determined on admission together with the classical prognostic variables. The relationship between Killip>I and subsequent post-discharge AMI was established with the Cox regression adapted for competitive events.
ResultsDuring a median follow-up of 3 years, 135 (13.9%) and 53 (12.4%) patients with Non-STE-ACS and STEMI presented a new AMI. Patients with Non-STE-ACS and STEMI with Killip>I (15.6% and 21.3% respectively) showed a higher incidence of AMI (28.3 vs 6.3 and 10.6 vs 3.3 per 100 patients-years of follow-up, p<0.001, respectively). In the multivariate analysis, adjusted for traditional risk factors and controlled for competitive events (death and revascularization), confirmed that Killip>I subjects with Non-STE-ACS and STEMI showed a significantly higher risk of AMI (HR: 1.76; CI 95%: 1.15-2.68; p=0.009 and HR: 1.90; 95% CI: 1.07-3.36; p=0.029 respectively).
ConclusionsIn patients with Non-STE-ACS and STEMI, the presence of Killip>I on admission is independently associated to an increased risk of long-term AMI.
Artículo
Diríjase desde aquí a la web de la >>>FESEMI<<< e inicie sesión mediante el formulario que se encuentra en la barra superior, pulsando sobre el candado.

Una vez autentificado, en la misma web de FESEMI, en el menú superior, elija la opción deseada.

>>>FESEMI<<<