

Es escasa la información de estudios cardiovasculares longitudinales. En hipertensos (HTA) y/o hipercolesterolémicos (HCL) españoles, con mal control inicial de la presión arterial (PA) y/o del colesterol total (CT) se cuantifica la tasa de incidencia (TI), la incidencia acumulada (IA), los riesgos relativos (RR), las curvas de supervivencia (CS), el cumplimiento terapéutico (CU) y se ajusta la escala de Framingham-Anderson (FA) a nuestro entorno.
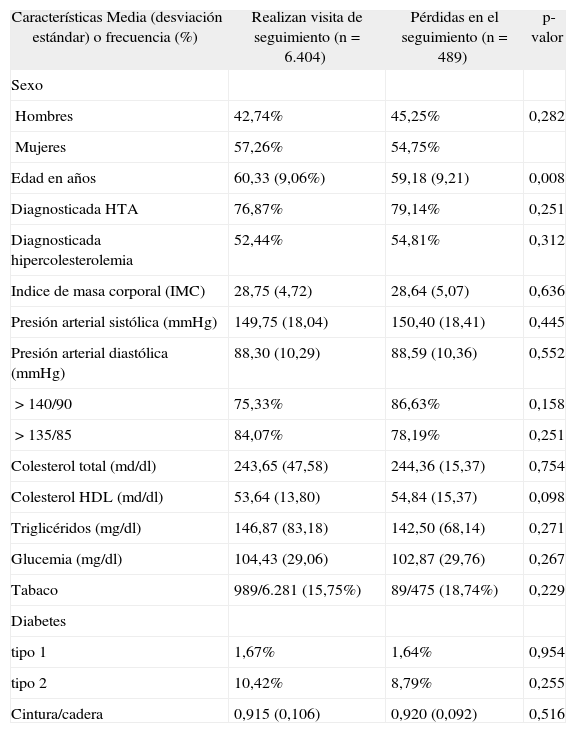
Pacientes y métodosSe analizaron 6.893 HTA y/o HCL en prevención primaria que aportaron un promedio de 1,22 años de seguimiento. Participaron 480 médicos. Se calcularon: la TI, IA y los RR; el método de Kaplan-Meier para la CS; Haynes-Sackett adaptado para el CU; el ajuste de FA por la recta de los mínimos cuadrados, coeficiente de correlación de Pearson (r) e intraclase (cci).
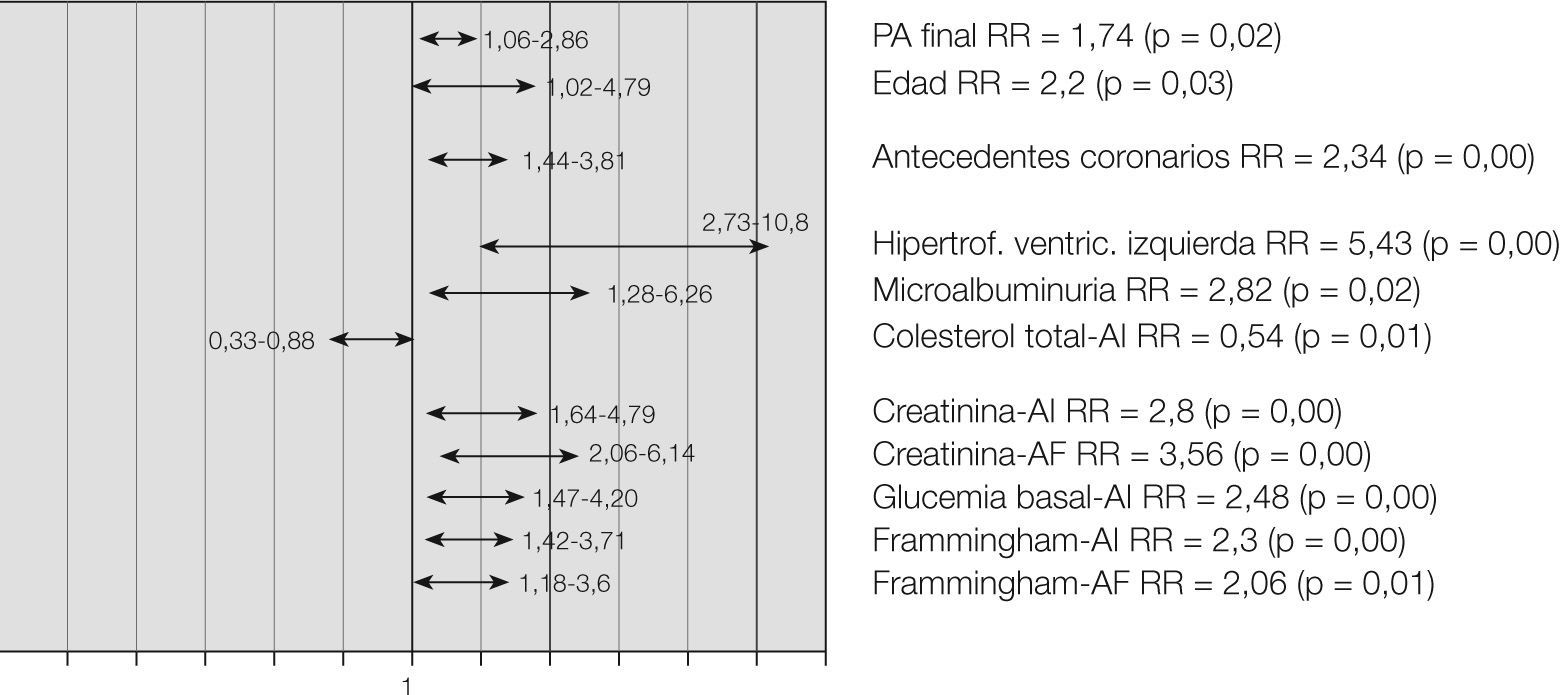
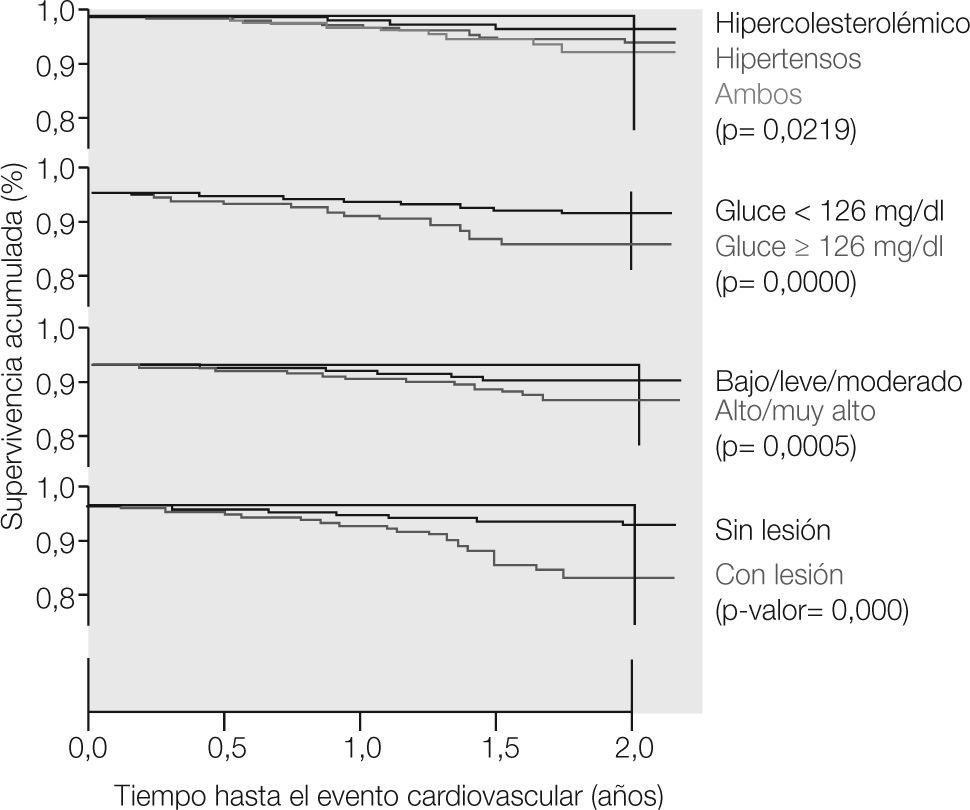
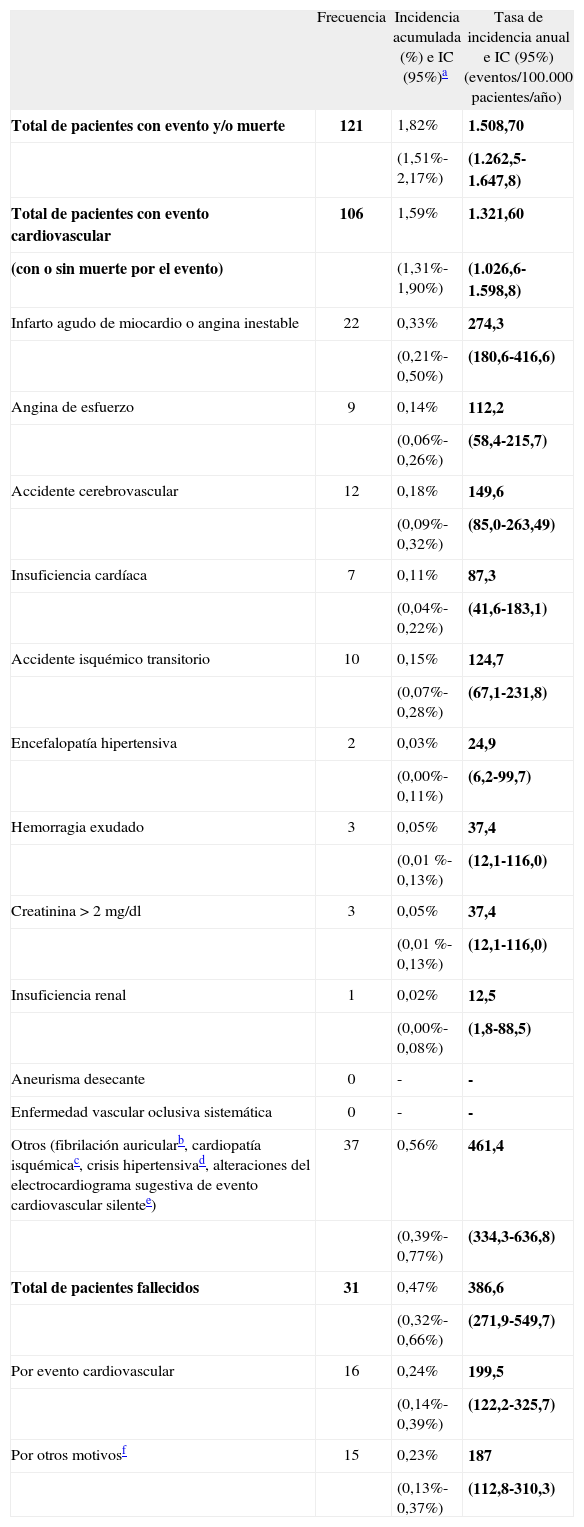
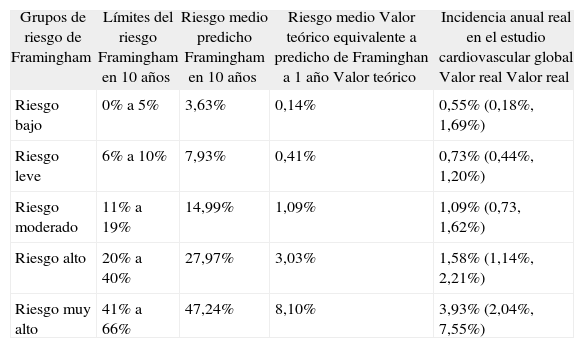
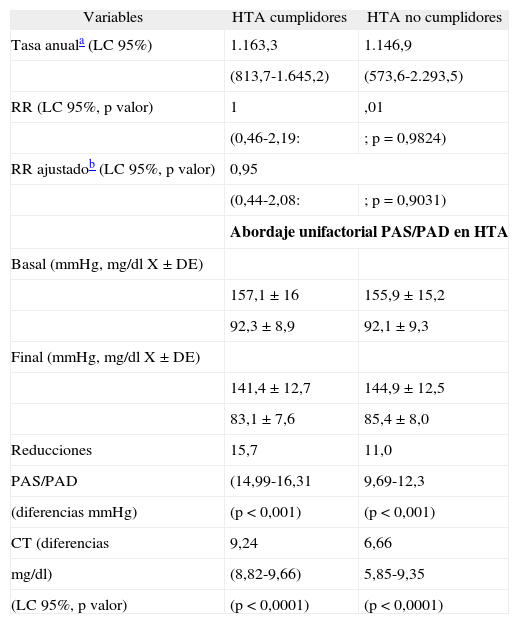
ResultadosLa IA fue 1,59% (1,31-1,90); la TI de 1.321, 6 eventos cardiovasculares por 100.000 pacientes/año (1.026,6-1.598,8). Los RR significativos fueron: edad (p=0,03), PA final (p=0,02), antecedentes coronarios (p=0,00), hipertrofia ventricular izquierda (HVI) (p=0,00), microalbuminuria (p=0,02), CT=250mg/dl al inicio (p=0,01), glucemia basal (Gb)≥126mg/dl al inicio (p=0,00), creatinina≥1,2mg/dl al inicio (p=0,00) y final (p =0,00), y no CU en HCL (p=0,00). Las CS realizadas por antecedentes de HTA y/o HCL, existencia o no de Gb≥126mg/dl, existencia o no de lesión de órganos diana, y tener o no riesgo cardiovascular (RCV) alto con FA, fueron significativas (p<0,05). El ajuste del FA para RCV global fue: (0,415 × Riesgo FA%) + 0,517%, obtuvo una r=0,9962 (p=0,00) y un cci=0,9969 (p<0,0001).
ConclusionesSe ajustó la ecuación FA en nuestros pacientes, con datos propios. Se cuantificaron los factores pronósticos y CS. Se cuantificó un beneficio entre CU y disminución de RCV en HCL.
There is little information on cardiovascular longitudinal studies. In Spanish patients with hypertension (AHT)) and/or hypercholesterolemia (HC), with poor initial control of blood pressure (BP) and/or total cholesterol (TC), incidence rate (IR), cumulative incidence (CI), relative risks (RR), survival curves (SC), therapeutic compliance (TC) were quantified and the Framingham-Anderson scale (FAS) was adjusted to our patients.
Patients and MethodsA total of 6,893 primary prevention patients with AHT and/or with HC were included in primary prevention, with an average of 1.22 years of follow-up. A total of 480 physicians participated. Incidence rate (IR), cumulative incidence (CIN), relative risks (RR), survival curves (SC) by Kaplan-Meier method, and therapeutic compliance (TCOM) by Haynes-Sackett self-reported questionnaire were calculated. The Framingham-Anderson scale (FAS) was validated with Pearson's correlation coefficient (r) and intraclass correlation index (ICI).
ResultsCIN was 1.59% (1.31-1.90); the IR 1,321.6 cardiovascular events/ 100,000 patients/year (1,026.6-1,598.8). RRs with statistical significance were: age (p=0.03). Blood pressure at the end of the study (p=0.02), coronary background (p=0.00), left ventricular hypertrophy (LVH) (p=0.00), microalbuminuria (p=0.02), CT≥250mg/dl (p=0.01), fasting glycemia (Gb)≥126mg/dl (p=0.00), creatinine≥1.2mg/dl at the beginning (p=0.00) and at the end of the study (p=0.00), and poor compliance in HC patients (p=0.00). SC have statistical significance (p<0.05) for AHT background, fasting glucose≥126mg/dl, target organ damage, and high cardiovascular risk with FAS scale. The adjusted FAS formula for global cardiovascular risk was (0.415 x FAS Risk%) + 0.517%, r=0.9962 (p=0.00) and ICI=0.9969 (p<0.0001).
ConclusionsThe equation for the FAS scale was adjusted for Spanish AHT/HC patients. Prognostic factors and SC were calculated. Benefitbetween TC and decrease of CVR in HC patients was quantified.
Article
Diríjase desde aquí a la web de la >>>FESEMI<<< e inicie sesión mediante el formulario que se encuentra en la barra superior, pulsando sobre el candado.

Una vez autentificado, en la misma web de FESEMI, en el menú superior, elija la opción deseada.

>>>FESEMI<<<


