
Given the increasing adoption of clinical ultrasound in medicine, it is essential to standardize its application, training, and research.
Objectives and methodsThe purpose of this document is to provide consensus recommendations to address questions about the practice and operation of clinical ultrasound units. Nineteen experts and leaders from advanced clinical ultrasound units participated. A modified Delphi consensus method was used.
ResultsA total of 137 consensus statements, based on evidence and expert opinion, were considered. The statements were distributed across 10 areas, and 99 recommendations achieved consensus.
ConclusionsThis consensus defines the most important aspects of clinical ultrasound in the field of Internal Medicine, with the aim of standardizing and promoting this healthcare advancement in its various aspects. The document has been prepared by the Clinical Ultrasound Working Group and endorsed by the Spanish Society of Internal Medicine.
Dada la creciente adopción de la ecografía clínica en medicina, es fundamental estandarizar su aplicación, formación e investigación.
Objetivos y métodosEl propósito de este documento es proporcionar recomendaciones de consenso para responder cuestiones sobre la práctica y el funcionamiento de las unidades de ecografía clínica. Participaron 19 expertos y responsables de unidades avanzadas de ecografía clínica. Se utilizó un método de consenso Delphi modificado.
ResultadosSe consideraron un total de 137 declaraciones de consenso, basadas en la evidencia y opinión experta. Las declaraciones fueron distribuidas en 10 áreas. 99 recomendaciones alcanzaron consenso.
ConclusionesEste consenso define los aspectos más importantes de la ecografía clínica en el ámbito de la Medicina Interna, con el objetivo de homogeneizar y promover este avance asistencial en sus diferentes vertientes. El documento ha sido elaborado por el Grupo de Trabajo de Ecografía Clínica y avalado por la Sociedad Española de Medicina Interna.
In recent years, ultrasound has been incorporated as an essential and commonly used tool in the clinical practice of internists, providing added value in patient care in a multitude of clinical contexts.1,2 For more than a decade, a growing number of Internal Medicine services have incorporated ultrasound into their regular clinical practice, in addition to developing teaching and research activities, through various organizational systems.3
Given the rapid growth in the use of this technique,4,5 the Clinical Ultrasound Working Group of the Spanish Society of Internal Medicine (GTEco-SEMI) has considered it necessary to establish some basic recommendations for the incorporation of this technique—healthcare advancement in its different aspects. For this purpose, this consensus document has been developed, which seeks to answer questions about the practice and operation of ultrasound units, taking into account the different organizational models. The objective of these recommendations is:
- -
Define the concept of clinical ultrasound and areas of application in Internal Medicine.
- -
Establish the criteria to develop the different aspects of care, teaching and research in clinical ultrasound in Internal Medicine services.
- -
Homogenize, ensure quality and promote the systematic use of clinical ultrasound.
- -
Structure training in clinical ultrasound for all specialists in Internal Medicine.
- -
Establish criteria in relation to the quality of clinical ultrasound studies performed by specialists in Internal Medicine.
- -
Facilitate the implementation of clinical ultrasound in new services or units.
- -
Define the necessary resources to facilitate the efficient development and maintenance of training programs for physicians, residents and medical students.
- -
Promote collaborative research in clinical ultrasound.
- -
Promote cooperation and constructive comparison of different units.
- -
Transfer these recommendations to the institutions in which the service or unit is integrated and to external agents.
The Ultrasound Group of the Spanish Society of Internal Medicine (GTEco-SEMI) brought together professionals with extensive experience in the founding and promotion of these specialized units. Several members of the GTEco-SEMI held a meeting within the XXIII Meeting of SEMI Internal Medicine Service and Unit Heads, held in Granada (Spain) on September 22, 2023. They raised the need to design a management document consensus to harmonize the practical application of clinical ultrasound, based on the most up-to-date scientific evidence through a MEDLINE search and with the national representation of internists with experience and knowledge in ultrasound, as well as the management of ultrasound units.
A group of 19 experts was selected, made up of those responsible for advanced clinical ultrasound units according to the SEMI-Excellent accreditation program6 (DGG, DT, GGCS, JCL, JTM, JOO, LBR, MMB, MMG, MTA, MBW, PVG, SMG, SLP, YTC), advisory members of the GTEco-SEMI board of directors (DGG, DT, GGCS, GS, JCL, JMO, JTM, LBF, LBR, MMB, MTA, MBW, SGR, PMR). In addition, two members representing the SEMI board of directors (JMP, MMB) and the outgoing coordinator of the ultrasound group of the European Federation of Internal Medicine (JTM) joined, but they participated in an individual capacity as experts, not as representatives of the society. The meeting was facilitated by the GTEco-SEMI (YTC) coordinator, with experience, postdoctoral training in education and research in clinical ultrasound.
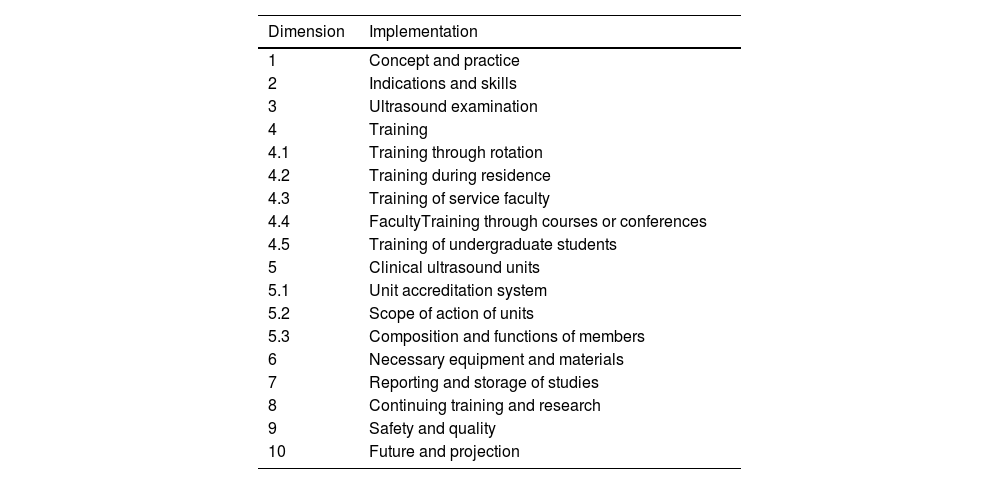
ResultsA literature search published in MEDLINE was performed using the keywords [“Point-of-Care Ultrasonography”], [“Clinical Ultrasonography”] or [“Bedside Ultrasonography”], presenting a draft of 137 statements on the recommendations that should be followed for the practical application of Clinical Ultrasound in Internal Medicine. This draft addressed aspects such as its definition, purposes and application examples, and was structured in 10 categories and ordered according to relevance, under the direction of the coordinator (YTC) [Table 1].
Dimensions considered for the recommendations included in the consensus.
| Dimension | Implementation |
|---|---|
| 1 | Concept and practice |
| 2 | Indications and skills |
| 3 | Ultrasound examination |
| 4 | Training |
| 4.1 | Training through rotation |
| 4.2 | Training during residence |
| 4.3 | Training of service faculty |
| 4.4 | FacultyTraining through courses or conferences |
| 4.5 | Training of undergraduate students |
| 5 | Clinical ultrasound units |
| 5.1 | Unit accreditation system |
| 5.2 | Scope of action of units |
| 5.3 | Composition and functions of members |
| 6 | Necessary equipment and materials |
| 7 | Reporting and storage of studies |
| 8 | Continuing training and research |
| 9 | Safety and quality |
| 10 | Future and projection |
Group members carefully evaluated these proposals to include their input and considerations. It was agreed to discard those that were outside the scope of the document as they were not feasible taking into account the different areas of professional practice of internists in our health system. Those recommendations in which 100% consensus was not obtained were discussed jointly in a first meeting of the group of experts, where it was determined to modify or exclude them.
This first meeting was convened through the Zoom Meetings® platform on October 10, which was facilitated by the coordinator (YTC) and two internists with experience in quality care (JTM, SGR). 29 statements were discarded, ultimately leaving a list of 108 statements.
After this meeting, participants were provided with a review of the validated Likert voting scale: 1 (totally disagree), 5 (neutral), and 9 (totally agree). It was planned to carry out no more than two rounds of online voting with the Google-Forms® tool. All votes were carried out confidentially, including all initial participants. The methodology classifies the statements as “consensus” (average ≥ 7 and deviation ≤ 1 of 2 points from the average), “almost consensus” (average ≥ 6.5 and deviation ≤ 2 of 2 points from the average) or “no consensus” (average <6.5 or deviation ≥ 3 of 2 points from the average).
In the second meeting held on October 19, 2023, the 78 statements that achieved consensus were stated. The 30 indicators that reached “near consensus” were reviewed to determine if they should be modified to improve the level of agreement and added to the next Delphi Survey or omitted entirely. 7 proposals were discarded, and the rest were discussed, refining 23. These were reviewed by two members (YTC, SGR), they made the appropriate modifications to the statement of the indicators, based on the comments shared by the participants and supported by the recording of the session and supplementary notes taken during the initial meeting, to ensure that all opinions were taken into account.
In this second vote, in which all members participated, 23 indicators were considered, achieving consensus on 21 statements. A final list of 99 proposed declarations is presented in Annex 1 (Supplementary material).
DiscussionBased on the results of our consensus, we recommend that these 99 statements (Annex 1 in Supplementary material) be considered essential for the implementation of clinical ultrasound in Internal Medicine.
These statements can serve the purpose of standardizing the application, training and research in ultrasound, while ensuring the competence and quality of the examinations performed.
Below we describe the most notable aspects of the consensus document.
Dimension 1. Concept and practiceStatements 1 to 12
Clinical ultrasound is defined as the systematic application of ultrasound as part of the physical examination (along with inspection, palpation, percussion and auscultation),7 in addition to being a tool that facilitates diagnosis, prognostic stratification, the monitoring and follow-up of people treated by specialists in internal medicine.8
Clinical ultrasound should be routinely integrated into the decision-making process in Internal Medicine, given its versatility and ability to provide detailed, real-time information at the patient's bedside.2 Performed, interpreted and incorporated into the care process by the appropriately trained and trained professional who cares for the patient, it is a fundamental added value competency in the practice of Internal Medicine,1,2 helping to optimize the management and distribution of resources.8 It significantly improves the diagnostic capabilities of doctors, allowing rapid and more accurate evaluations without the need to transport patients to other services, being safe and widely available.1,2
Its scope of application in Internal Medicine continues to expand, contributing to better care and outcomes for patients in various clinical situations.
Dimension 2. Indications and skillsStatements 13 to 16
The objective of basic skills is to recognize normal anatomy and function, differentiating them from pathological situations. 28 core competencies in ultrasound have been identified and are shown in Annex 1 (Section 2.2 in Supplementary material).
Ultrasound can also be used in the diagnostic approach based on the patient's symptoms or signs in different clinical scenarios, identifying 16 competencies that are described in Annex 1 (Section 2.3 in Supplementary material).
This list of competencies can be expanded according to the evidence and technological advances of each moment, its widespread use within the specialty and its profitability, as well as its application in monographic consultations (autoimmune diseases, thromboembolic disease, cardiovascular risk, etc.).5
Dimension 3. Ultrasound examinationStatements 17 to 22
In the same way that the internist offers comprehensive care and a holistic approach, ultrasound training should also be based on these principles.1,2
A multi-organ ultrasound examination is proposed with selected basic planes of the lung, heart and abdomen that should be done systematically in the evaluation of all patients. The diagnostic profitability of the selected ultrasound planes has been demonstrated in multiple studies.2,9
Dimension 4. TrainingStatements 23 to 54
There are an increasing number of training programs in Clinical Ultrasound available for internists.2,10 Training in each center must be developed, establishing minimum necessary criteria, depending on the size of the unit, service, the habitual use of ultrasound and institutional resources.
It is important to highlight that success in the development of a training program in accordance with the proposed guidelines requires significant institutional support and the endorsement of scientific societies is recommended.10
It is recommended to develop a certification process in this competence, to guarantee adequate quality in the application of this tool for the benefit of our patients.
Training through rotation (1 month)
Statements 26 to 32
There are different rotation programs in ultrasound in Internal Medicine.3 Dimension 4.2 shows the minimum standards that must be addressed in a specific ultrasound rotation, depending on the level of training and experience. Structured theoretical and practical training must be followed by a competency assessment.11
Each rotator must perform approximately 150 supervised scans during the rotation period. The use of simulators helps to ensure that homogeneous exposure to different pathologies is provided.12
Training during residence
Statements 33 to 35
During the residency period, a progressive acquisition of competence is recommended, and an initial one-month rotation may be useful to learn basic knowledge and skills, followed by continuous training within the curriculum, to reinforce learning and acquire more skills advanced.
Training of service faculty
Statements 36 to 41
As long as the rotation (1 month), previously described, is not available, other methodologies are recommended for the adapted and flexible training of physicians.13
It is necessary to define appropriate and specific learning objectives for each physician, with the creation of specifically designed courses, and integrate this training within the work day, respecting clinical care and the proper functioning of the service. Daily supervised examination shifts with the unit's teaching staff are recommended.
Training through courses or conferences
Statements 42 to 51
These recommendations are based on strategies that seek to improve an effective learning experience focused on the individual needs of each student.14
Educational materials should be provided before and after the course to reinforce learning. The ratio between students and instructors in the practical part should not be greater than 5 to 1 to ensure adequate training in skills, maximizing exploration time by the student.13
Training of undergraduate students
Statements 52 to 53
The incorporation of ultrasound in undergraduate training is a reality in many universities.12 Teaching basic clinical ultrasound facilitates training in Anatomy, Physiology and Pathophysiology, but, above all, improves the performance and reliability of the physical examination. This requires planning and sufficient human and material resources for the training of a large number of students. With the expansion of ultrasound to multiple specialties, teaching during undergraduate training is essential, and the role of general specialties is key.12
It is recommended that internists with skills in clinical ultrasound and university teaching activity collaborate in teaching this skill through elective subjects, seminars or clinical practice.
Dimension 5. Clinical ultrasound unitsUnit accreditation system
Statements 54 to 57
It is essential to establish a training accreditation system for the performance, teaching and research in clinical ultrasound of Internal Medicine services, such as those included in the SEMI-EXCELENTE accreditation program.6 According to different criteria of structure, organization and management, the clinical ultrasound unit can be classified as healthcare, teaching or advanced.
The fundamental objectives of the SEMI-EXCELENTE accreditation system are:
- •
Ensure the training and quality of the examinations performed for the benefit of the patient
- •
Homogenize, ensure quality and promote teaching in clinical ultrasound.
- •
Facilitate the implementation of clinical ultrasound in new services or units.
- •
Promote collaborative research in clinical ultrasound.
- •
Prepare a National Registry of accredited services or units.
Setting
Statements 58 to 60
In addition to its proven usefulness in conventional hospitalization, other specialty care settings (day hospitals, outpatient clinics, home hospitalization, home palliative care) benefit from this technique.9
Composition and functions of the members
Statements 61 to 65
Internists who are dedicated to providing care, teaching and research in clinical ultrasound must have clinical skills, given that correct interpretation depends on the assessment of their results in a well-defined clinical context. In addition, you must have accredited experience in clinical ultrasound, as well as sufficient time for assistance and teaching (depending on the type of unit). At least 1–2 members of the unit, (depending on the number of people to be trained), must be dedicated to the development of the training program.
Dimension 6. Equipment and materialsStatements 66 to 70
It is essential to have suitable ultrasound machines, equipped with at least one convex, sector and linear probe, or failing that, with a multi-frequency probe, that are continuously available. The creation of an ultrasound unit must be a strategic project of the service and the health institution where it takes place and the investment must be ensured to be able to have materials of appropriate quality for its proper functioning.13
Dimension 7. Reporting and storage of studiesStatements 71 to 76
Clinical ultrasound involves a quantifiable healthcare activity with clinical impact, and therefore it is essential that a clinical note be generated in the patient's history whenever it is performed. The design and implementation of a form for the systematic collection of information is recommended.
Recording images and videos is desirable for legal, investigative and auditing purposes. The clinical ultrasound core competency report should be included in the medical record after the physical examination, preferably in a dichotomous manner, indicating that the ultrasound was performed by an internist and only reporting on aspects related to specific defined competencies.
Dimension 8. Continuous training and researchStatements 77 to 81
It is advisable to periodically meet with unit members, continue training to acquire new skills and techniques, as well as review cases of special interest.
Promoting high-quality research is a priority, preferably with multicenter studies and clinical trials focused on improving the patient's diagnosis, therapy or prognosis.5
Dimension 9. Security and qualityStatements 82 to 92
Clinical ultrasound in expert hands represents an excellent tool to increase diagnostic certainty, allows the establishment of therapeutic measures and helps reduce the risk associated with performing certain invasive procedures.13
Ultrasound users must follow standard safety practices, including ALARA (As Low As Reasonably Achievable — the minimum exposure that allows a quality study), equipment maintenance and decontamination of probes, promoting measures that avoid associated nosocomial infections.13,15
Dimension 10. ForecastStatements 93 to 99
Constantly evolving technological, educational, and practical advancement can offer new approaches, efficiencies, and modalities in the care of our patients.5
This consensus document addresses a wide variety of elements, trying to answer questions about the adequate implementation of clinical ultrasound in Internal Medicine services. From the working group, we consider that it may be useful to have a document that offers general guidance, with the aim of standardizing and promoting the incorporation of this technique.
This work has several limitations. First, given that the incorporation of ultrasound in Internal Medicine is relatively recent, most of the literature reviewed was from the emergency field, accentuating the need to promote collaborative research in our services. Secondly, the members of the expert group had extensive knowledge in ultrasound, although not necessarily in all the areas developed in this consensus, encouraging diversity and different points of view. And lastly, some of the statements are subjective perceptions, with no studies to support their practice at the moment, so monitoring will have to be carried out, establishing periodic updates as new evidence emerges.
ConclusionThe Spanish Society of Internal Medicine and the Clinical Ultrasound Working Group, after an initial stage of expansion of clinical ultrasound in Spain, reiterate their recommendation to incorporate this technique in all Internal Medicine services without exceptions. It is essential, to achieve this goal, to establish a set of guidelines that are reflected in this document, addressing the key points regarding the execution and structure of the various organizational modalities of the ultrasound units. These guidelines are the guide for healthcare activity, teaching and research; and they aim to guarantee the adequate training of professionals, as well as the excellence of the examinations carried out, with the purpose of standardizing and promoting the incorporation of this healthcare advance in its different aspects.
FundingThis research has not received specific support from public sector agencies, the commercial sector or non-profit entities.
Conflicts of interestThe authors declare that they have no conflict of interest.
EthicsWe certify that this research has been carried out in accordance with the ethical principles of our institution. This work and tables have not been previously published and reproduced from another source. No ethical approval was required or applied for this work.
Data access and accountabilityYale Tung Chen, principal investigator of the study, had full access to all data and takes responsibility for the integrity and accuracy of the data analysis.
The following is Supplementary data to this article:

